

Abstract
Keywords: Family medicine, chronic wound, wound care, debridement, dressing materials
Introduction
Chronic wound healing, regardless of etiological origin, is a complex pathological process in which normal wound-healing stages fail to be completed within the expected timeframe, and such wounds are often prone to infection and biofilm formation (1). This condition, increasingly recognized as a global health concern, affects approximately 40 million people and, despite advances in modern medical technologies, imposes a difficult-to-sustain economic burden on healthcare systems due to its treatment-resistant nature. In particular, the rapidly increasing aging population, together with accompanying comorbidities such as diabetes and hypertension and broader demographic changes, is driving the prevalence of chronic wounds toward what has been described as a "silent pandemic" (2).
Chronic wounds are defined as wounds that do not follow the normal healing process and generally fail to heal within four to six weeks (3). These wounds often remain in the inflammatory phase (4). It is estimated that 1–2% of the global population will experience a chronic wound during their lifetime (5). Factors such as diabetes, venous hypertension, peripheral artery disease, poor nutrition, wound bed hypoxia, and infection contribute to the chronicity of wounds (6). While the normal healing process consists of hemostasis, inflammation, proliferation, and maturation phases, this balance is disrupted in chronic wounds (7). In chronic wound management, debridement of necrotic tissue, infection control, maintenance of appropriate moisture balance, and pressure relief are fundamental steps (8). Treatment may involve modern dressing materials, such as hydrocolloids, alginates, and hydrogels, or advanced methods, such as negative-pressure wound therapy, depending on the wound characteristics. One of the key factors exacerbating the problem is the reduction of chronic wound management to simple wound dressing and the lack of a multidisciplinary approach. Although primary healthcare services represent a strategic component in managing this problem, the competence of family physicians in current debridement techniques, wound-bed preparation (TIME [Tissue, Infection/Inflammation, Moisture, Edge] and TIMERS [Tissue, Infection/Inflammation, Moisture, Edge, Repair/Regeneration, Social factors] frameworks), and modern dressing materials remains a subject of debate. Nonstandardized diagnosis and treatment approaches may result in prolonged healing times, costly complications, and deterioration in patients' quality of life.
Primary healthcare services play a critical role in the early diagnosis, treatment, and patient education processes of chronic wounds. Improving family physicians' knowledge in this area may enhance patient outcomes and help reduce the burden on the healthcare system (9).
This study aimed to evaluate the knowledge levels and clinical approaches of family physicians regarding chronic wound care, including debridement management, infection control, and current dressing materials.
Materials and Methods
The population of this descriptive study consisted of 470 contracted family physicians working in Manisa province, Türkiye. During the research process, we aimed to recruit as many family physicians as possible who agreed to participate in the study within the specified dates.
Some of the family physicians declined to participate, and the research was completed with the participation of family physicians who volunteered for the study. The overall participation rate was 86.2%. The study protocol was approved by the Manisa Celal Bayar University Faculty of Medicine Health Sciences Ethics Committee on September 6, 2023 (No: 20.478.486/987).
Data were collected using a 93-item knowledge questionnaire. The first section included questions on the demographic and occupational characteristics of the participants, and the second section covered the knowledge of chronic wound management, including the TIMERS framework, general wound care, dressing, and wound types (diabetic, venous, ischemic, and pressure ulcers).
In evaluating the knowledge questionnaire, 1 point was awarded for each correct response, and 0 points were assigned for incorrect or unanswered items. The raw scores were converted to a 100-point scale (number of correct responses / total number of questions × 100) and standardized as the "knowledge success score" to facilitate comparative analysis. Data were collected after obtaining written informed consent from the participants.
Data were analyzed using IBM SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were expressed as numbers (n), percentages (%), means ± standard deviations (SD), and medians (minimum–maximum). The normality of numerical data was assessed using the Shapiro-Wilk test.
For comparisons between two groups, the independent samples t-test was used when the data were normally distributed, and the Mann-Whitney U test was used when they were not. Cronbach’s α coefficients were calculated to assess scale reliability and internal consistency. The competency levels and knowledge gaps of physicians in chronic wound management were visualized using a radar chart (spider chart). A p-value < 0.05 was considered statistically significant.
Results
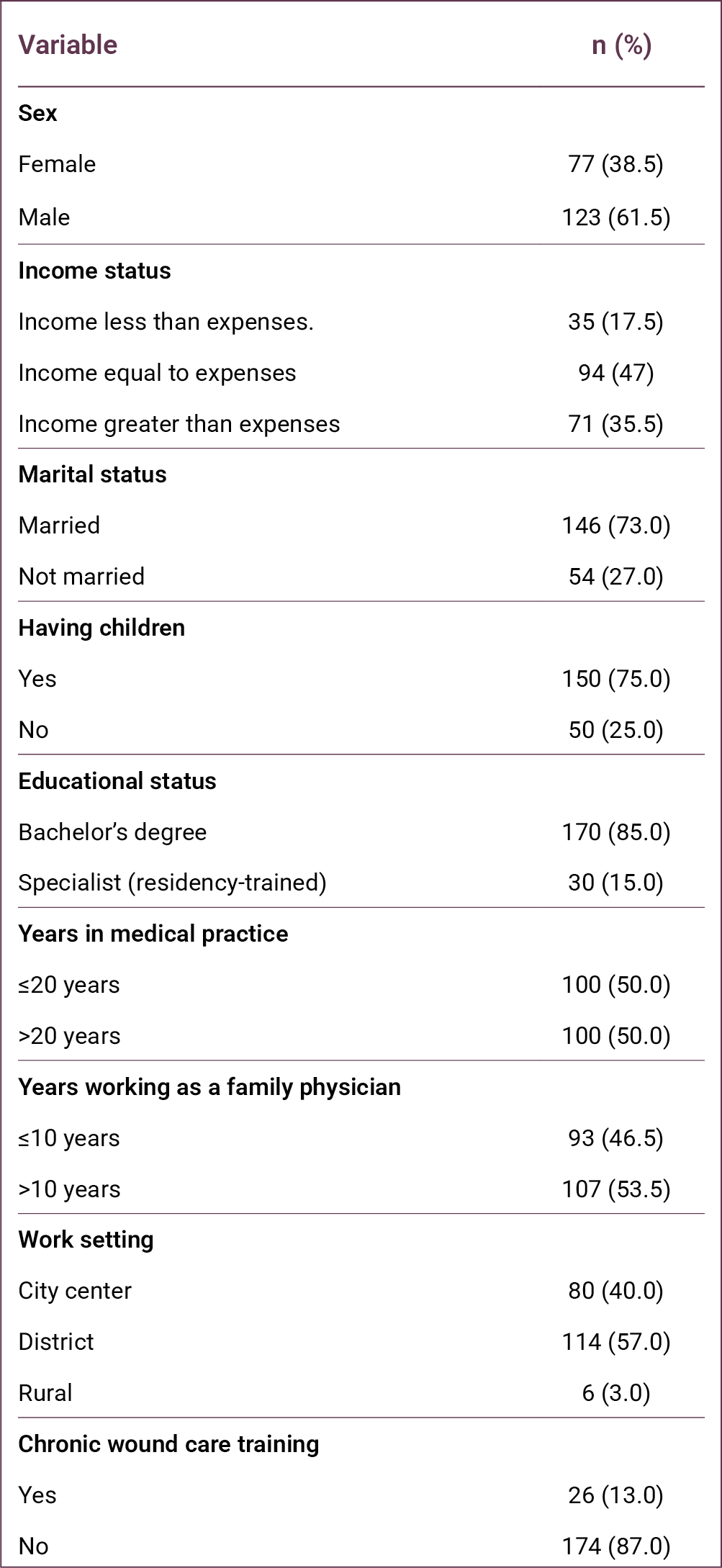
The study was conducted with 200 family physicians among the 470 working in Manisa province. Of the participants, 123 (61.5%) were male, 146 (73%) were married, 150 (75%) had children, and 156 (78%) lived with their spouse or children. Regarding economic status, 94 (47%) reported that their income was equal to their expenses. In terms of professional status, 157 (78.5%) were general practitioners, 13 (6.5%) were family medicine residents working under contract, and 30 (15%) were family medicine specialists. Only 26 (13%) physicians had received training in wound care (Table 1).
Women physicians had a higher mean number of correct responses (61.25 ± 18.41) compared with male physicians (56.93 ± 21.26). Physicians with a bachelor's degree answered 57.81 ± 20.32 questions correctly, whereas those with specialist training answered 63.03 ± 19.73 questions correctly. Physicians working in the city center answered 56.56 ± 20.40 questions correctly, while those working in districts and rural areas answered 59.95 ± 20.16 questions correctly.
When years of professional experience were examined, physicians with ≤20 years of experience answered 59.31 ± 20.04 questions correctly, while those with >20 years of experience answered 57.89 ± 20.57 questions correctly. Similarly, based on years of experience in family medicine, physicians with ≤10 years of experience answered 57.87 ± 21.66 questions correctly, while those with >10 years of experience answered 59.23 ± 19.07 questions correctly.
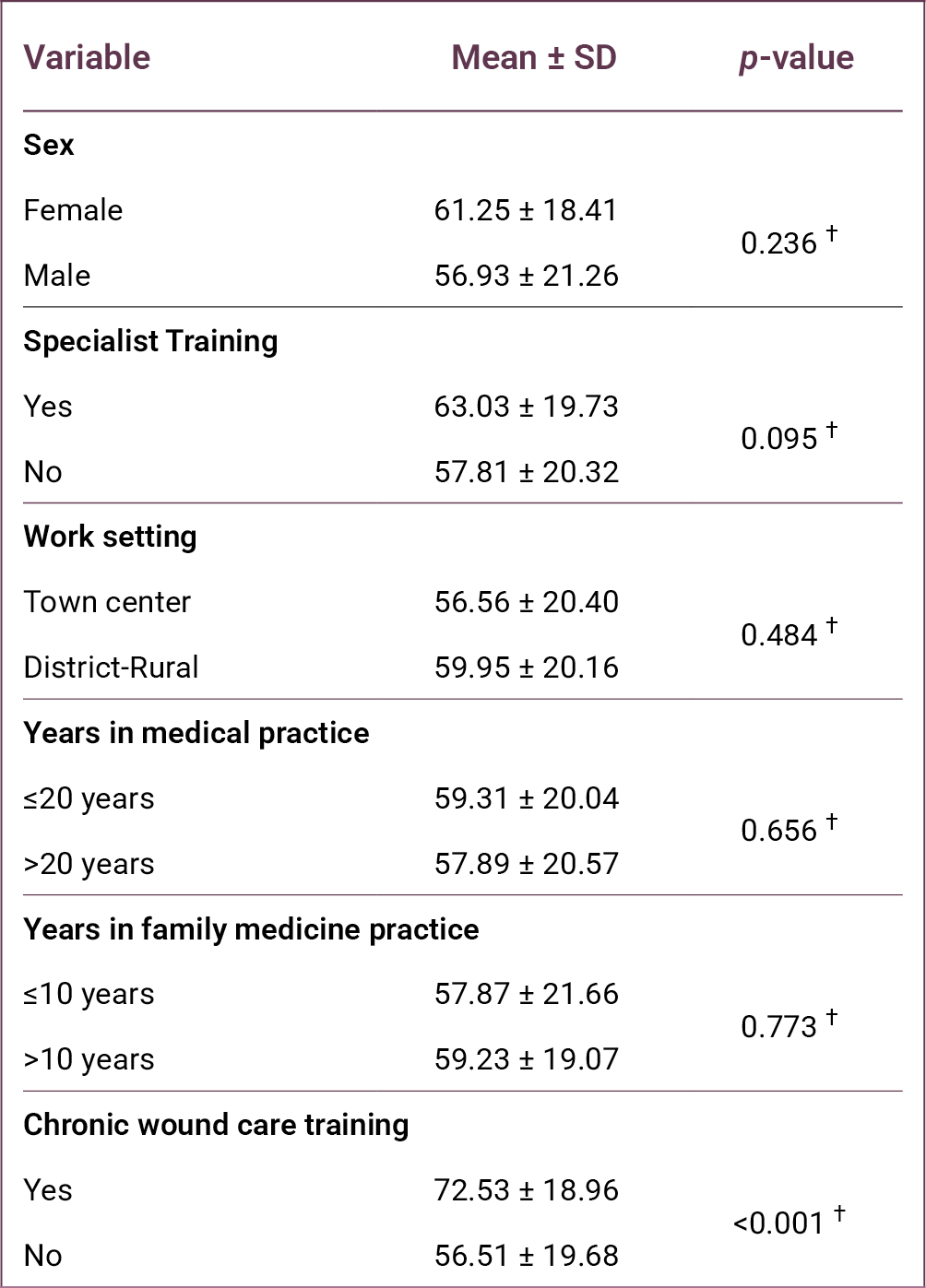
Among all variables examined, only the difference associated with wound care training was statistically significant (p < 0.001). Physicians who had received chronic wound care training answered 72.53 ± 18.96 questions correctly, whereas those without such training answered 56.51 ± 19.68 questions correctly.
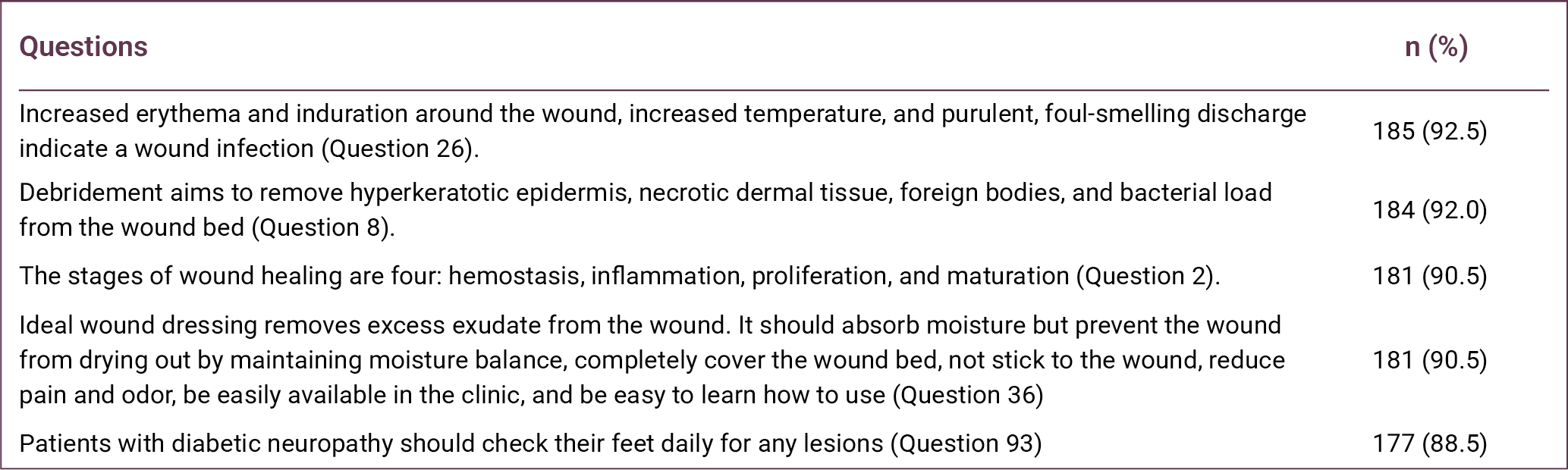
Question 26, regarding indicators of wound infection, had the highest number of correct responses (n = 185). This was followed by Question 8, which assessed knowledge of the purpose of debridement (n = 184). Question 2, related to the stages of wound healing, ranked third with 181 correct responses (Table 3).
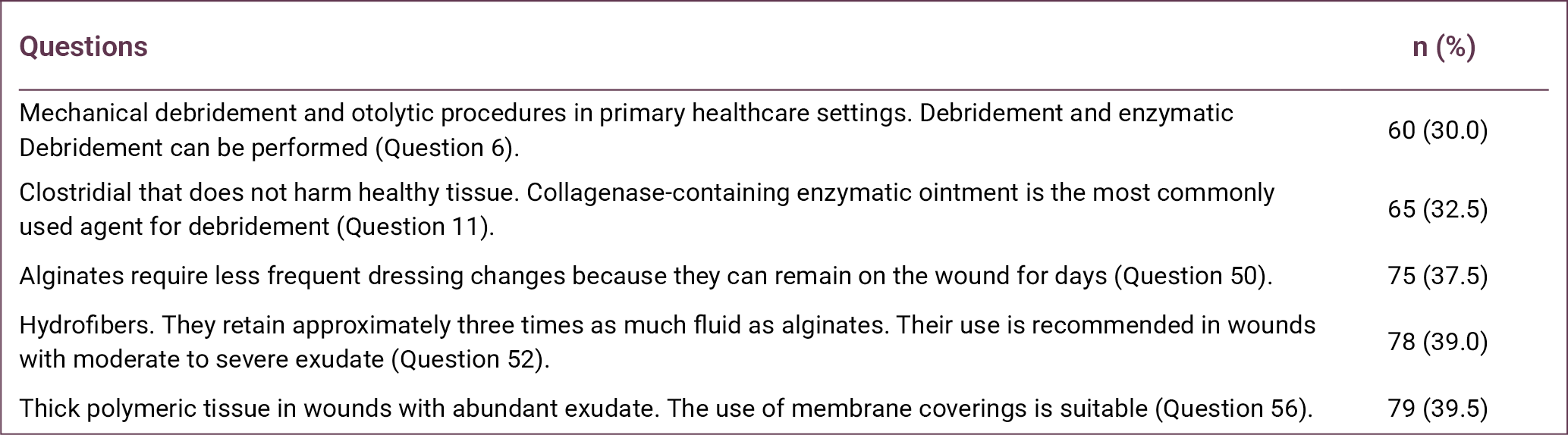
In contrast, Question 6, which addressed the types of debridement that can be performed in primary healthcare settings, had the lowest number of correct responses (n = 60). Question 11, concerning the most commonly used agent for enzymatic debridement, had the second lowest number of correct responses (n = 65). Question 50, regarding the replacement period of alginates, ranked third lowest with 75 correct responses (Table 4).
Reliability analyses of the subdimensions of the knowledge questionnaire used in the study are presented in Table 5. Cronbach’s α coefficients demonstrated high reliability for the subdimensions of wound care and dressing (0.929), venous wounds (0.850), and pressure ulcers (0.839). Acceptable reliability was observed for moisture balance (0.751), infection and inflammation (0.745), ischemic wounds (0.732), and debridement management (0.696).
Lower reliability values were observed for the chronic wound (0.387) and diabetic wound (0.505) subdimensions, likely due to the limited number of items in these categories. When the knowledge categories were examined, family physicians achieved the highest success rate in the chronic wound category (77.83%), whereas the lowest success rate was observed in the wound care and dressing category (54.05%).
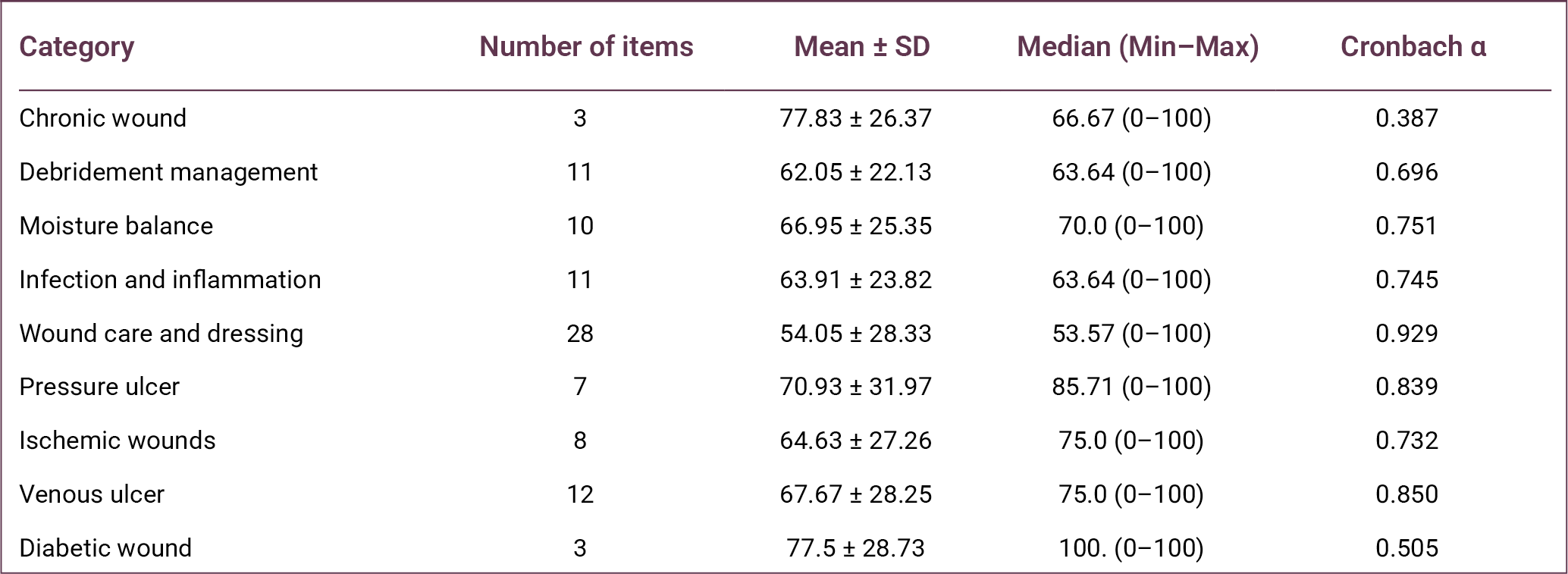
The radar (spider) chart presented in Figure 1 illustrates the distribution of family physicians’ competencies and knowledge gaps in chronic wound management. The chart demonstrates an asymmetrical distribution of knowledge across categories. The chronic wound category is positioned closest to the outer edge of the chart, indicating the highest level of knowledge. Conversely, the wound care and dressing category lies closest to the center, indicating the lowest level of performance.
The relationship between receiving chronic wound care training and knowledge scores is presented in Table 6. Physicians who had received training (n = 26) demonstrated significantly higher scores than those without training (n = 174) across nearly all categories.
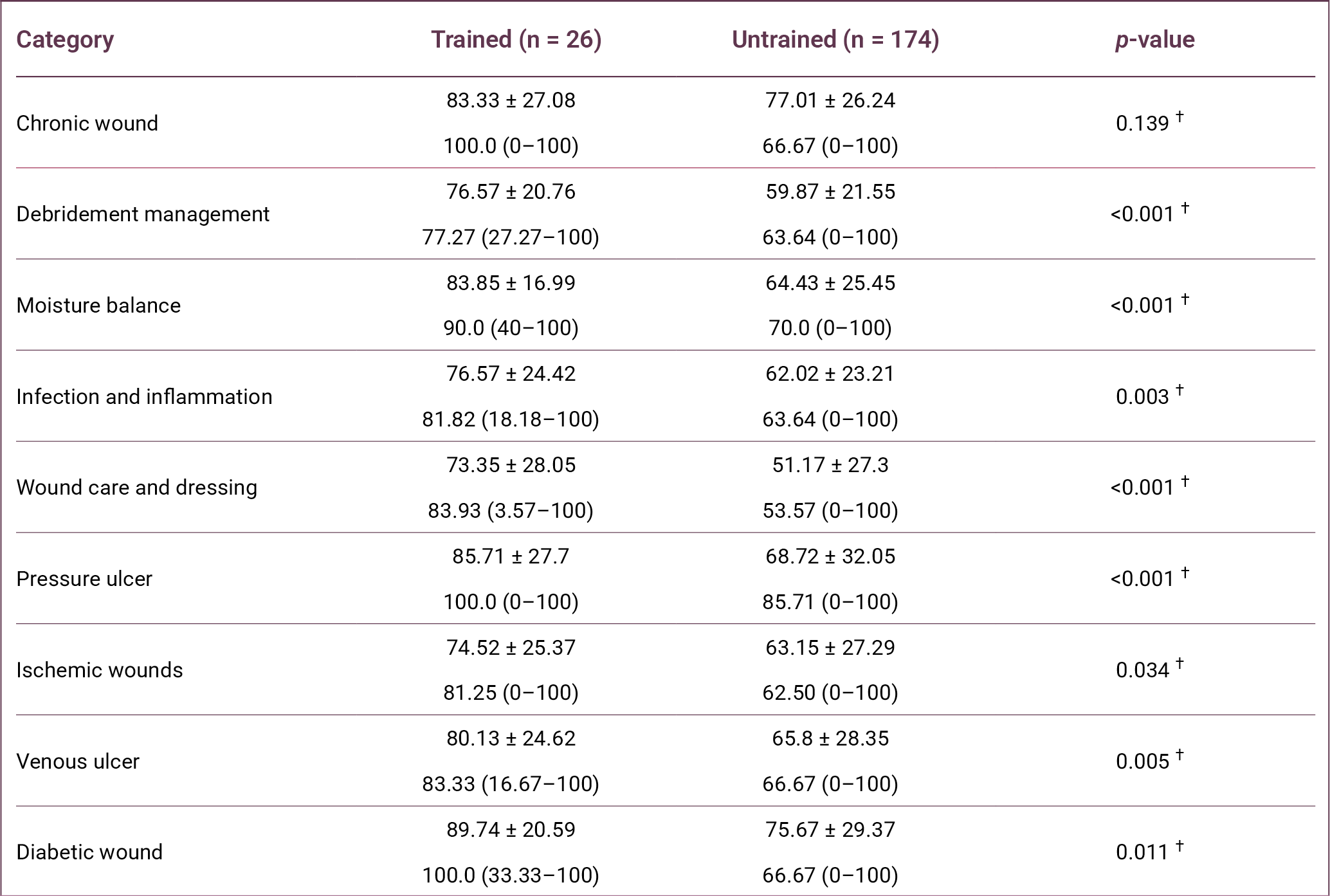
In the debridement management category, the success rate was 76.57% in the trained group and 59.87% in the untrained group (p < 0.001). In the moisture balance category, success rates were 83.85% in the trained group and 64.43% in the untrained group (p < 0.001).
In the wound care and dressing category, which showed the lowest overall success rate, the trained group achieved 73.35%, whereas the untrained group achieved 51.17% (p < 0.001). In the pressure ulcer category, the success rate in the trained group (85.71%) was also significantly higher than in the untrained group (68.72%) (p < 0.001).
Similarly, in the infection and inflammation category, physicians who received training scored significantly higher (76.57%) than those without training (62.02%) (p = 0.003). In the vascular and diabetic wound categories, trained physicians also demonstrated significantly higher knowledge levels in venous wounds (p = 0.005), ischemic wounds (p = 0.034), and diabetic wounds (p = 0.011).
However, in the chronic wound definition category, the difference between the trained group (83.33%) and the untrained group (77.01%) was not statistically significant (p = 0.139).
Discussion
This study evaluated the competencies and clinical approaches of family physicians, who play a central role in primary healthcare services, in chronic wound care, debridement management, infection control, and the use of current dressing materials. The findings indicate that family physicians demonstrate a high level of awareness regarding the recognition and the general definition of chronic wounds, but substantial knowledge gaps remain in practical management and technical interventions.
Chronic wounds represent a major clinical and economic burden for healthcare systems and significantly impair patients' quality of life. Since no single medical specialty is responsible for the management of chronic wounds, their care requires a multidisciplinary approach involving multiple levels of the healthcare system.
Family medicine is a comprehensive medical specialty that provides continuous, person-centered care across all age groups and health conditions, integrating clinical and behavioral sciences while remaining easily accessible within the community (10). Within this framework, family physicians often represent the first point of contact for patients presenting with chronic wounds, placing them in a key position for early assessment and initial management. Therefore, strengthening wound care competencies in primary care is essential and necessitates the development of structured training programs.
Adequate wound care training enables physicians to perform appropriate wound assessment, initiate evidence-based treatment, and identify cases requiring referral to specialized care. Timely and effective wound management at the primary care level may reduce unnecessary referrals to secondary and tertiary healthcare services while improving patient outcomes.
In this study, the knowledge levels of family physicians regarding chronic wound management were examined, and the significant impact of training status on knowledge and competency levels was demonstrated. The finding that only 13% of participants had received wound care training highlights a substantial educational gap in primary healthcare settings.
Consistent with our findings, the study by Şahan et al. (11) reported that only 19 (10.67%) participants had received wound care training within the previous four years. In the present study, wound care training was associated with significantly higher knowledge scores, particularly in areas requiring technical competence such as debridement management (p < 0.001), moisture balance (p < 0.001), and wound care and dressing practices (p < 0.001).
Similarly, the study by Fernández-Araque et al. (12) demonstrated that greater exposure to wound care training was associated with improved knowledge levels. Şahan et al. (11) also reported a statistically significant relationship between wound care training and knowledge test performance.
The finding that physicians without training achieved only a 51.17% success rate in the dressing materials category suggests that modern wound management approaches, such as hydrocolloids and silver-containing dressings, may not be sufficiently integrated into routine clinical practice (11).
This study has several limitations. First, it was conducted among family physicians working in a single province, and therefore, the findings may not be generalizable to all primary care physicians in Türkiye. Second, data were collected using a self-report questionnaire that primarily reflects participants' theoretical knowledge rather than their clinical practice. Finally, the cross-sectional study design prevents the establishment of causal relationships between the variables examined.
In conclusion, effective chronic wound management in primary healthcare requires not only the ability to recognize and classify wounds but also sufficient knowledge of modern wound care interventions and dressing materials. The findings of this study indicate that important knowledge gaps persist in the practical management of chronic wounds among family physicians. Expanding wound care training programs and integrating structured wound management education into undergraduate medical curricula and family medicine residency training may help strengthen physicians’ competencies and improve the quality of chronic wound care in primary healthcare settings.
REFERENCES
Öztaş P. [Wound healing, care, and treatment]. Ankara Eğt Arş Hast Derg. 2021;54(2):341–51. Turkish. [CrossRef]
Las Heras K, Igartua M, Santos-Vizcaino E, Hernandez RM. Chronic wounds: Current status, available strategies and emerging therapeutic solutions. J Control Release. 2020;328:532–50. [CrossRef]
Graves N, Phillips CJ, Harding K. A narrative review of the epidemiology and economics of chronic wounds. Br J Dermatol. 2022;187(2):141–8. [CrossRef]
Raziyeva K, Kim Y, Zharkinbekov Z, Kassymbek K, Jimi S, Saparov A. Immunology of acute and chronic wound healing. Biomolecules. 2021;11(5):700. [CrossRef]
Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Adv Wound Care (New Rochelle). 2021;10(5):281–92. [CrossRef]
Eriksson E, Liu PY, Schultz GS, Martins-Green MM, Tanaka R, Weir D, et al. Chronic wounds: Treatment consensus. Wound Repair Regen. 2022;30(2):156–71. Erratum in: Wound Repair Regen. 2022;30(4):536. [CrossRef]
Verdolino DV, Thomason HA, Fotticchia A, Cartmell S. Wound dressings: curbing inflammation in chronic wound healing. Emerg Top Life Sci. 2021;5(4):523–37. [CrossRef]
Mongkornwong A, Wongwiwat W, Chansanti O, Sukprasert P, Akaranuchat N. Hard-to-heal wounds. PSU Medical Journal, 2024;1-12.
Akman M. [The strength of primary care in Türkiye]. Türk Aile Hek Derg. 2014;18(2):70–8. Turkish.
Edwards D, Black AT, Spielfogel WD. A multidisciplinary approach to managing ischemic wounds and current treatment options. Curr Treat Options Cardio Med. 2021;23(7):51. [CrossRef]
Şahan S and Harputlu D. [Determining the knowledge levels of primary healthcare workers regarding chronic wound care]. Etkili Hemşirelik Derg. 2025;18(2): 250–61. Turkish. [CrossRef]
Fernández-Araque A, Martinez-Delgado M, Jiménez JM, López M, Castro MJ, Gila EC. Assessment of nurses' level of knowledge of the management of chronic wounds. Nurse Educ Today. 2024;134:106084. [CrossRef]